- Summary
- Symptoms
- Read More
Summary
Gout is a form of crystal deposition arthritis, hence the name gouty arthritis. Uric acid, a chemical that is found in the serum component of our blood, and a by-product of protein metabolism, is the key chemical that contributes to gout. In a liquid form, uric acid is an essential component of normal metabolism. The painful symptoms of gout occur when uric acid changes from a liquid to a solid. This transformation from a liquid to a crystal occurs with a drop in body temperature. Excessively high levels of uric acid lead to the deposition of monosodium urate crystals into joints and certain subcutaneous spaces in the body that are close to the skin and affected by variations in body temperature. Gout is found more commonly in men than in women. Gout is usually found in men between the ages of 40 and 70 years.
Symptoms
- Acute onset of severe pain, typically at night
- Location of gout attack may vary, but most common site is the great toe joint
- Intense erythema (redness) and edema (swelling) is found
- Pain usually subsides in a matter of days
Description
 Gout, also called podagra, is a form of arthritis that affects 1-2% of the western population. Gout is a crystal deposition disease that can be easily described by this example: as children, we would make our own rock candy. We'd get a pot of water and begin to heat it on the stove. As the water warmed, we'd add sugar. The hotter the water became, the more sugar we could dissolve. When the water was close to a boil and saturated with sugar, we would remove it from the heat and allow the sugar to crystallize on a string as the water cooled. The crystallization of the sugar was due to high concentrations of sugar that could not be supported in solution as the temperature of the water cooled. Acute gouty attacks are due to the same crystallization process.
Gout, also called podagra, is a form of arthritis that affects 1-2% of the western population. Gout is a crystal deposition disease that can be easily described by this example: as children, we would make our own rock candy. We'd get a pot of water and begin to heat it on the stove. As the water warmed, we'd add sugar. The hotter the water became, the more sugar we could dissolve. When the water was close to a boil and saturated with sugar, we would remove it from the heat and allow the sugar to crystallize on a string as the water cooled. The crystallization of the sugar was due to high concentrations of sugar that could not be supported in solution as the temperature of the water cooled. Acute gouty attacks are due to the same crystallization process.
 Most acute gouty attacks occur in the late hours of the night. As we sleep, our bodies tend to focus on the primary metabolic functions such as digestion, breathing, etc. The extremities, such as the feet, tend to cool as a result of this decrease in circulatory flow. As they cool, and if the dissolved amount of uric acid is high enough, the result is the change of uric acid from a liquid to a crystal. The three hallmark symptoms of gout are that the onset is at night, the pain is severe, and the pain is specific to the great toe joint.(1) Gout occurs in the great toe joint in more than 50% of all gout cases. (2)
Most acute gouty attacks occur in the late hours of the night. As we sleep, our bodies tend to focus on the primary metabolic functions such as digestion, breathing, etc. The extremities, such as the feet, tend to cool as a result of this decrease in circulatory flow. As they cool, and if the dissolved amount of uric acid is high enough, the result is the change of uric acid from a liquid to a crystal. The three hallmark symptoms of gout are that the onset is at night, the pain is severe, and the pain is specific to the great toe joint.(1) Gout occurs in the great toe joint in more than 50% of all gout cases. (2)
Uric acid is measured in the serum (liquid) component of our blood. Normal levels of uric acid for men are less than 7mg/dl of serum and slightly less for most women. This level tends to rise in women following menopause. The vast majority of gout patients are men with an onset during the 4th to 5th decade of life. If serum uric acid levels surpass 10mg/dl, the likelihood of a gout attack is very probable.
Causes and contributing factors
High levels of uric acid (hyperuricemia) result from poor excretion of uric acid by the kidneys or by excessive production of uric acid based on dietary intake. 90% of all cases of gout are the result of underexcretion of uric acid. (3) Ten percent of all patients who have hyperuricemia will experience gout during their lifetimes. (4) The inability to metabolize purines may be inherited or acquired. (5) Purines are protein components in foods that are found commonly in the following foods:
following foods:
Heavy red meats and organ parts (sausage, liver, kidney, tongue, heart)
Dark fillet fish (mackerel, anchovies, sardines, herring and fish roe)
Peanuts
Alcohol
Dairy products (milk, ice cream, cottage cheese)
Fructose sweetened drinks
Individuals who have had acute gouty attacks should limit their intake of these foods.(4,6) This does not mean that they need to completely eliminate these foods from their diets, but rather they should consume these foods with moderation. Serum uric acid is also significantly influenced by the ability of the kidney to excrete uric acid. Factors that may change normal renal function may result in limited excretion of uric acid. These factors include the use of thiazide (HCTZ -hydrochlorthizide) diuretic therapy, dehydration, and renal failure. Many antihypertensive (blood pressure lowering) medications include HCTZ and include Dyazide, Maxide, Moduretic, indapamide, Microzide, and Zaroxolyn. Low doses of HCTZ do not seem to increase the risk of gouty attack. (7) Additional medications that may contribute to gout include niacin and aspirin. (6) Other factors that may contribute to the onset of gout include trauma, the stress of surgery, emotional stress, fatigue, infection or the use of penicillin.
Obesity is also a contributing factor to hyperuricemia, noting that a body mass equal to or greater than 35 results in a three times greater chance of gouty attacks. (4)
Differential diagnosis
The differential diagnosis for gout includes:
Arthritis
Bunion
Freiberg's infraction
Hallux limitus
Hallux rigidus
Pseudogout
Rheumatoid arthritis
Septic arthritis
Sesamoiditis
Sesamoid fracture
The diagnosis of gout can be confirmed with aspiration of synovial fluid from the affected joint. Distinctive uric acid crystals can be identified with microscopic fluid analysis.
Treatment
The most significant consideration in the treatment of gout is the frequency of attacks. Frequent attacks (more than once a year) will result in progressive erosion of the joint, leading to painful chronic arthritis. Isolated attacks (less than once a year) lead to minimal destruction of the joint. The frequency of gouty attacks determines whether treatment is merely for each individual attack, or whether daily medication should be taken to lower levels of serum uric acid.
(more than once a year) will result in progressive erosion of the joint, leading to painful chronic arthritis. Isolated attacks (less than once a year) lead to minimal destruction of the joint. The frequency of gouty attacks determines whether treatment is merely for each individual attack, or whether daily medication should be taken to lower levels of serum uric acid.
Methods used to prevent gouty attacks include weight loss, reduction of foods that may contribute to gout, and increased consumption of vitamin C. Daily consumption of 1500mg of vitamin C decreases the risk of gout by 45%. (8)
Treatment of an acute gout attack includes the use of prednisone or non-steroidal anti-inflammatory medications such as Indocin or Clinoril. Control of pain may require a mild narcotic such as codeine. Other treatment may include Colchicine (Colcrys) which yields dramatic results but carries severe side effects which include nausea and severe diarrhea. Colchicine is dosed once every two hours until the desired (or undesired) effects are achieved.
Recurrent attacks of gout in patients with hyperuricemia are common and occur greater than once each year in more than 60% of patients with hyperuricemia. (9) Treatment of recurrent attacks includes modifications in diet as previously discussed and the use of Allopurinal (Zylorpim), an inhibitor of uric acid synthesis. Probenecid is also used to increase the output of uric acid by the kidney. Dosing and combination therapy depends upon the level of serum uric acid which is measured periodically during therapy. Individuals prone to gouty attacks should also maintain a high fluid intake to promote the excretion of uric acid and decrease the tendency to form uric acid stones in the kidney and bladder. Uloric (febuxostat) is another medication that may be used as an alternative to Allopurinal.
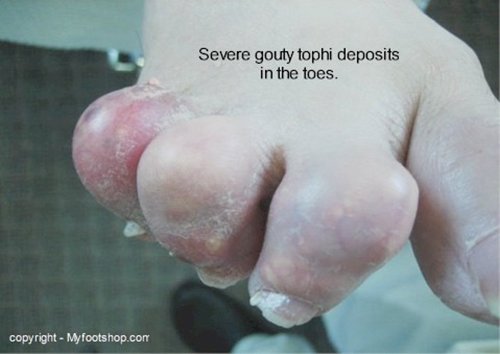
Gouty arthritis is the sequela of multiple untreated attacks that progressively destroy the cartilage of the joint. Surgical debridement of a joint with chronic damaged by chronic gout shows depositions of a material called gouty tophi that resemble cottage cheese. Gouty tophi erode the surface cartilage of the joint, resulting in premature destruction of the joint. Debridement of the joint, fusion or joint replacement is often indicated. (5)
When to contact your doctor
Acute and chronic gout should be managed by your doctor to prevent destruction of the joint. Contact your local podiatrist or orthopedist for additional information on the treatment of gout.
References
1. Chen LX, Schumacher HR (October 2008). "Gout: an evidence-based review". J Clin Rheumatol 14 (5 Suppl): S55–62.doi:10.1097/RHU.0b013e3181896921
2. Schlesinger N (March 2010). "Diagnosing and treating gout: a review to aid primary care physicians". Postgrad Med 122 (2): 157–61.doi:10.3810/pgm.2010.03.2133. PMID 20203467
3. Vitart V, Rudan I, Hayward C et al. (April 2008). "SLC2A9 is a newly identified urate transporter influencing serum urate concentration, urate excretion and gout". Nat. Genet.40 (4): 437–42. doi:10.1038/ng.106
4. Weaver, AL (July 2008). "Epidemiology of gout". Cleveland Clinic journal of medicine. 75 Suppl 5: S9–12. doi:10.3949/ccjm.75.Suppl_5.S9
5. Richette P, Bardin T (January 2010). "Gout". Lancet 375 (9711): 318–28. doi:10.1016/S0140-6736(09)60883-7
6. Terkeltaub R (January 2010). "Update on gout: new therapeutic strategies and options". Nature Reviews Rheumatology 6 (1): 30–8.doi:10.1038/nrrheum.2009.236
7. Laubscher T, Dumont Z, Regier L, Jensen B (December 2009). "Taking the stress out of managing gout". Can Fam Physician 55 (12): 1209–12. PMC 2793228
8. Choi HK, Gao X, Curhan G (March 2009). "Vitamin C intake and the risk of gout in men: a prospective study". Arch. Intern. Med. 169 (5): 502–7.doi:10.1001/archinternmed.2008.606
9. Eggebeen AT (2007). "Gout: an update". Am Fam Physician 76 (6): 801–8. PMID 17910294
Author(s) and date
![]() This article was written by Myfootshop.com medical advisor Jeffrey A. Oster, DPM.
This article was written by Myfootshop.com medical advisor Jeffrey A. Oster, DPM.
Competing Interests - None
Cite this article as: Oster, Jeffrey. Gout https://www.myfootshop.com/article/gout
Most recent article update: December 10, 2020.
 Gout by Myfootshop.com is licensed under a Creative Commons Attribution-NonCommercial 3.0 Unported License.
Gout by Myfootshop.com is licensed under a Creative Commons Attribution-NonCommercial 3.0 Unported License.
Internal reference only: ZoneP5, ZoneD7, ZoneL11, ZoneM9














