





Lisfranc fracture-dislocation benefits from Carbon Fiber Insoles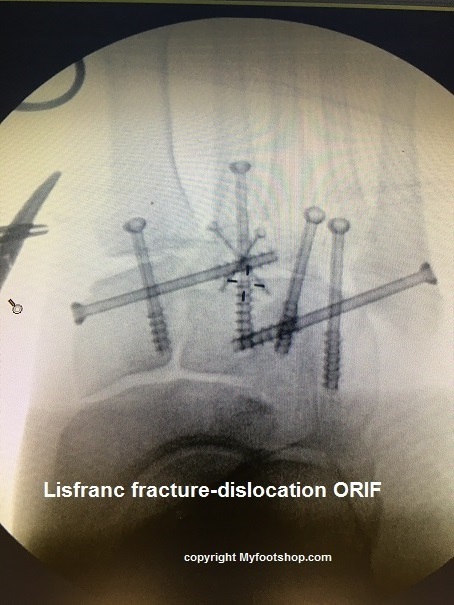
Working in a rural hospital I see a lot of foot and ankle trauma. ATV and motor sports injuries are common and often result in midfoot injuries. When the trauma is specific to the tarsal-metatarsal joint, we call these injuries Lisfranc dislocations or Lisfranc fractures. Jacques Lisfranc de St. Martin (1790-1847) was a French surgeon and gynecologist (a Jacques of all trades) who recognized this injury while treating soldiers of the Napoleonic Wars. These unique fractures and dislocations continue to bear his name to this date.
Lisfranc injuries are defined by classic fracture patterns including the Quenu and Kuss classification and the Hardcastle classification. (1,2) Unfortunately, these classifications do not dictate the long term outcomes of theses fractures and dislocations. Lisfranc fracture-dislocations can be devastating injuries with lifelong disability. Many patients who sustain these injuries are unable to return to their prior occupations and recreational activities. Long term post traumatic arthritis is common in these cases and directly correlates to the success of anatomical reduction achieved at the time of surgery. (3)
Return to weight bearing and ambulation post Lisfranc fracture-dislocation
Walking can be described as a controlled forward fall. To move forward in walking, we shift our center of gravity forward and begin a forward fall. The function of the leg, ankle and foot is to act as a lever to manage that forward fall in a controlled manner. The soleus muscle of the calf is designed to slowly limit range of motion at the ankle during walking. As our center of gravity moves forward, there is increasing and significant load applied to the midfoot and forefoot. In the patient who has sustained a Lisfranc fracture-dislocation, simple weight bearing is a load applied to the injury site in a perpendicular manner. The load applied to the foot by the soleus muscle to limit forward motion during walking is applied to Lisfranc’s joint perpendicular to the injury. When load is aligned with the direction of a fracture, the load can be distributed over a larger surface area. But when load is applied perpendicular to the injury, fatigue and failure of the fracture-dislocation site is common. This pattern of weight bearing and load bearing, perpendicular to the fracture-dislocation, is what makes return to activities such a challenge to Lisfranc fracture-dislocation patients.
What are the two ways a Carbon Fiber Spring Plate enables early return to walking?
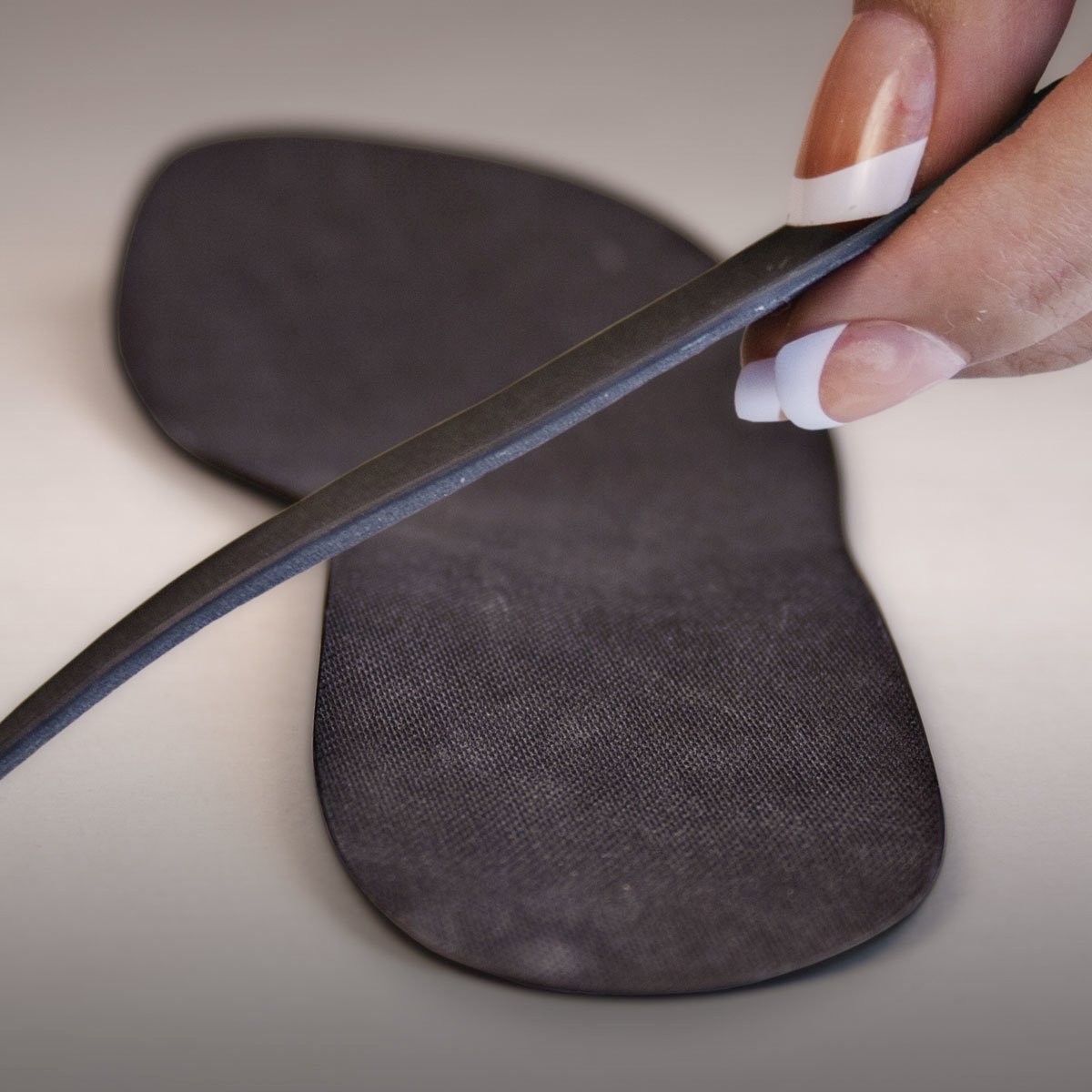 The first attribute of the Carbon Fiber Spring Plate is rigidity. Carbon Fiber Spring Plates are extremely thin and very, very rigid. The rigidity of the Spring Plate is an important part of Lisfranc fracture-dislocation and return to weight bearing. When combined with a traditional laced shoe (laced tennis shoe, laced walking shoe or laced boot) the Spring Plate become securely positioned on the bottom of the foot to received the force generated by the soleus muscle during walking. The combination of a Spring Plate and a laced shoe essentially becomes a Spring Plate Brace. Load generated by the soleus muscle is carried by the Spring Plate in a direction parallel to the line of force. The Lisfranc fracture-dislocation, perpendicular to the line of force, is splinted and protected by use of the Carbon Fiber Spring Plate.
The first attribute of the Carbon Fiber Spring Plate is rigidity. Carbon Fiber Spring Plates are extremely thin and very, very rigid. The rigidity of the Spring Plate is an important part of Lisfranc fracture-dislocation and return to weight bearing. When combined with a traditional laced shoe (laced tennis shoe, laced walking shoe or laced boot) the Spring Plate become securely positioned on the bottom of the foot to received the force generated by the soleus muscle during walking. The combination of a Spring Plate and a laced shoe essentially becomes a Spring Plate Brace. Load generated by the soleus muscle is carried by the Spring Plate in a direction parallel to the line of force. The Lisfranc fracture-dislocation, perpendicular to the line of force, is splinted and protected by use of the Carbon Fiber Spring Plate.
Toe spring is the second attribute of the Carbon Fiber Spring Plate that enables early return to ambulation post Lisfranc fracture-dislocation. Toe spring (also called an anterior rocker) describes a rounded surface of the insert under the ball-of–the-foot. Normal walking relies on the immovable, static position of the foot as the body passes over the foot. This progressive increase in load to the foot by the soleus muscle as the body’s center of mass moves forward results in significant mechanical load to the Lisfranc fracture-dislocation. Placing a Carbon Fiber Spring Plate with toe spring in the shoe significantly decreases the load to the fracture-dislocation. Rather than big mechanical load and explosive heel lift, the toe spring in the Carbon Fiber Spring Plate promotes gradual loading and gradual heel lift, thus reducing load to the fracture-dislocation.
Rigid carbon fiber and toe spring – off-loading of midfoot injuries
Rigidity of the Spring Plate carries mechanical load, toe spring decreases mechanical load and a laced shoe ties is all together. I call this combination a Carbon Fiber Spring Brace. A Carbon Fiber Spring Brace is useful not only in the early stage of rehabilitation post Lisfranc fracture-dislocation, but also for long term use. The usability of the Carbon Fiber Spring Brace is far superior to a rigid plastic AFO. The use of a Carbon Fiber Spring Plate/Brace is a significant part of my care for these patients. It enables early return to walking and maintains surgical reduction during the healing phase of these injuries. Knowing that many of these injuries will go on to have post traumatic midfoot arthritis, I continue to use the Carbon Fiber Spring Plate as a long term brace for management of midfoot, post-traumatic arthritis.
Join the discussion on this topic in our discussion forum.
Jeff

Medical Adviser
Myfootshop.com
- Quenu E, Kuss GE. Etude sur les luxations du metatarse (Luxations metatarso-tarsiennes). Du diastasis entre le 1er et le 2e metatarsien. Rev Chir. 1909;39:1–72.
- Hardcastle PH, Reschauer R, Kutscha-Lissberg E, Schoffmann W. Injuries to the tarsometatarsal joint: incidence, classification and treatment. J Bone Joint Surg Br. 1982;64:349–356.
- Myerson MS, Fisher RT, Burgess AR, Kenzora JE. Fracture dislocations of the tarsometatarsal joints: end results correlated with pathology and treatment. Foot Ankle. 1986;6:225–242.

XLT Carbon Fiber Spring Plate Graphite Insole

XAT Carbon Fiber Spring Plate Graphite Insoles




